The Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) convened a group of experts to publish an update to their 2010 C.difficile infection (CDI) guidelines. Below is a summary of the new guidelines from the perspective of an emergency medicine (EM) pharmacist.
Clostridioides is the new Clostridium
- While the new guidelines use the nomenclature Clostridium difficile, the Clinical & Laboratory Standards Institute Antimicrobial Susceptibility Testing documents have been updated to Clostridioides difficile. The good news is “C.diff” still applies.
Diagnosis
- A multi step algorithm is now recommended for diagnosis:1
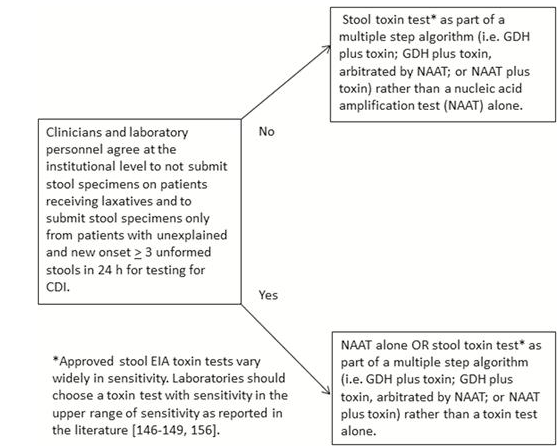
- Only patients with risk factors for CDI and ≥ 3 unformed stools in a 24 hour period should be tested
Pertinent Changes From Previous Guideline
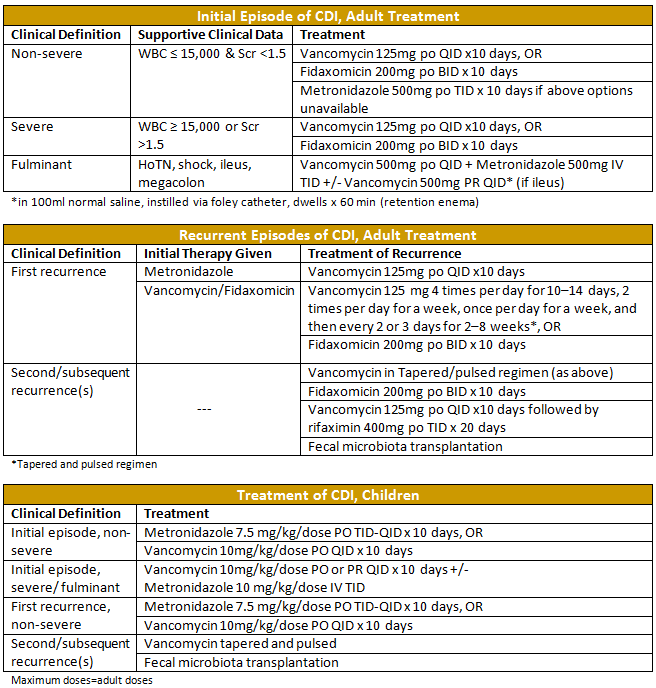
- Metronidazole is no longer recommended first line for any severity of CDI.
- This change is based on data to support vancomycin and fidaxomicin providing patients with a better chance of sustained symptom resolution one month after treatment.
- Serum creatinine (Scr) values for classification of severity is an absolute value rather than being compared to a change from baseline values
- Justification by the authors was that baseline values are often unavailable, which is certainly common in the ED setting, making the scoring easier for us to complete.
- For the first time fecal microbiota transplantation (FMT) is mentioned as a therapeutic option. Although not something that will be completed in the ED, it is something we should be aware of as this practice will continue to increase.
CDI Prevention & Control
- Antimicrobial Stewardship
- The most important modifiable risk factor for the development of CDI is exposure to antibiotic agents, making the appropriate use of antibiotics of paramount importance. The new guidelines flat-out recommend implementing a stewardship program. The ED is a great place for stewardship, ripe with opportunity, including decreasing CDI incidence.
- Consider restricting antibiotics that are most strongly associated with CDI such as fluoroquinolones, clindamycin, and broad-spectrum cephalosporins.
- Appropriate duration of therapy is also extremely important. There is a growing body of evidence for many infections that a shorter course of therapy than what has been historically used is equally efficacious. A great read on this is The New Antibiotic Mantra—“Shorter Is Better” by Dr. Brad Spellberg.2
- EM pharmacists have a unique opportunity to be major players in antimicrobial stewardship activities. We can potentially decrease the risk of CDI by advocating for patients and recommending narrower-spectrum antibiotics when appropriate. Additionally, we can recommend evidenced-based, appropriate durations for patients being discharged with an antibiotic prescription.
- Proton Pump Inhibitors (PPIs)
- There is an epidemiologic association between PPI use and CDI, though the authors of the guidelines felt there is insufficient evidence for discontinuing PPIs solely to prevent CDI.
- Avoiding the use of unnecessary PPIs, and using them for limited durations is never a bad idea.
- Probiotics
- Primary prevention- while there are multiple meta-analyses suggesting probiotics may prevent CDI in patients taking antibiotics, the data was not deemed sufficient to recommend their use.
- Secondary prevention- Saccharomyces boulardii (Florastor®) and Lactobacillus spp. (Culturelle®, Yakult®) may be of benefit to decrease CDI recurrence, although significant and reproducible results have yet to be shown in controlled trials.
- Ultimately, the data isn’t yet strong enough to make recommendations for or against. Probiotics are certainly not without risk, as the contents can cause invasive disease, and they can be costly.3 Last I checked, no one has died of a yogurt-related complication, so that is probably a safe recommendation to make.
- C.diff Scoring Tool
- While the new guidelines don’t make specific recommendations on the use of a predictive risk scoring system, such a tool would be very useful for identification of patients who would most benefit from risk mitigation.
- A study by Kuntz et al. produced such a tool that proved useful for stratifying CDI risk following an outpatient healthcare visit.4
- A more recent study by Reveles et al. produced a clinical prediction tool to be used to identify patients at high risk for CDI recurrence.5
Treatment Considerations
- Discontinue Systemic Antibiotics as Soon as Possible
- If discontinuing antibiotics isn’t possible, use the narrowest spectrum agent that will be effective.
- Patients with Active CDI Requiring Antibiotics
- One retrospective study has been published and suggests no benefit to extending anti-CDI therapy beyond 14 days for patients receiving concurrent systemic antibiotics. Relapse rates were similar for the regular and extended treatment groups in the univariate (17% and 23%, respectively; odds ratio [OR]: 1.4, 95% confidence interval [CI]: 0.7–2.7, p = 0.286) and multivariate analyses (OR: 0.7, 95% CI: 0.3–1.7, p = 0.425).6
- With only one retrospective study evaluating this topic, and minimal risk of extending therapy until after systemic antibiotics have been completed, many clinicians may still opt to do so. The new guidelines state that vancomycin 125mg PO daily may be sufficient to prevent recurrence after the initial course is complete.
- Patients Who Have Completed Anti-CDI Therapy and Now Require Antibiotics
- Two retrospective studies have been published that investigate the utility of giving oral vancomycin as secondary prophylaxis to patients requiring systemic antibiotics. Both studies showed decreased incidence of CDI for patients given prophylaxis.7,8
- One of these studies showed oral vancomycin prophylaxis decreased the risk of further recurrence in patients whose CDI itself was a recurrence (AHR, 0.47; 95% CI, 0.32–0.69; P<0.0001) but not in those whose CDI was an initial episode (AHR, 0.91; 95% CI, 0.57–1.45; P=0.68). This suggests patients with multiple recurrences of CDI will benefit most from prophylactic therapy when requiring systemic antibiotics.8
- While lacking prospective trials, it may be prudent to prophylax patients who have a history of CDI and now require systemic antibiotics with vancomycin 125mg PO daily. Patients with multiple recurrences may benefit most from this practice. While lacking data, metronidazole IV is an option when patients are unable to receive oral medications, but preference should be given to vancomycin when enteral administration is available.
- Antimotility Agents
- Historically, antimotility agents, such as loperamide, have been discouraged in CDI out of concern for worse outcomes like toxic megacolon. Koo et al. published a review article where they sought to study the literature to determine the basis of this practice. They found that all patients who experienced complications or died were given antimotility agents alone initially, without concurrent anti-CDI therapy. The authors of the new guidelines suggest that it may be safe to give antimotility agents adjunctively to patients also receiving anti-CDI therapy.9
- Intravenous Vancomycin
- IV vancomycin has no effect on CDI as it is not excreted appreciably into the colon and therefore is not discussed in this, or any other guideline as a therapeutic option.
- Duration of CDI Treatment
- Nearly all randomized trials utilized 10 day regimens which are usually sufficient.
- If patients improve but do not have symptom resolution at 10 days, extending the course to 14 days can be considered.
- If metronidazole is used, it should be limited to one course out of concern for neurotoxicity (including irreversible peripheral neuropathy) which has been associated with treatment durations > 4 weeks.10
- CDI Treatment Recommendations:
Logistics of First Line Therapy
- Vancomycin capsules and fidaxomicin are both expensive, and often not covered by insurance. Estimated cash prices are below.11
- Vancomycin 125mg PO capsules (40 caps) ~ $1,250.00
- Fidaxomicin 200mg PO capsules (20 caps) ~ $4,400.00
- Intravenous vancomycin is often utilized orally in the inpatient setting to minimize cost, and compounding pharmacies may offer more affordable options using this method. However, compounding pharmacies typically have limited hours and often retail pharmacies do not have compounding capabilities which can make this option difficult.
- FIRVANQTM, a commercially manufactured vancomycin oral liquid has recently been approved by the FDA. Per their website, CutisPharma is targeting a launch date of April 2, 2018. We will have to wait to see how much FIRVANQ costs to ultimately determine its role, though a commercially available, reasonably priced vancomycin liquid is appealing.
Take Home Points
- IDSA/SHEA have released new CDI guidelines.
- Emergency medicine pharmacists should play a huge role in antimicrobial stewardship, which is a key component in minimizing the occurrence of CDI.
- Vancomycin PO or fidaxomicin are now the recommended first line agents for CDI, however, the high cost associated with these therapies may prohibit their use in some patients.
- Metronidazole should only be considered when vancomycin PO or fidaxomicin are unavailable for adults. It is still a first line option for children.
- Vancomycin PO therapy may be extended in patients with active CDI, or used prophylactically in patients with previous CDI episodes to prevent recurrent infection while on systemic antibiotics.
- FIRVANQTM, a new oral liquid vancomycin formation, will soon be available, but cost information is currently unknown.
Tony Mixon, PharmD, BCPS
Emergency Medicine/Infectious Disease Clinical Pharmacist
Peer reviewed by:
Craig Cocchio, PharmD, BCPS
References
- McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Disease. 2018.
- Spellberg B. The New Antibiotic Mantra-“Shorter Is Better”. JAMA Intern Med. 2016 Sep 1;176(9):1254-5.
- Gouriet F, Million M, Henri M, Fournier PE, Raoult D. Lactobacillus rhamnosus bacteremia: an emerging clinical entity. Eur J Clin Microbiol Infect Dis 2012; 31:2469–80.
- Kuntz JL, Johnson ES, Raebel MA. Predicting the risk of Clostridium difficile infection following an outpatient visit: development and external validation of a pragmatic, prognostic risk score. Clin Microbiol Infect. 2015 Mar;21(3):256-62
- Reveles KR, Mortensen EM, Koeller JM et al. Derivation and Validation of a Clostridium difficile Infection Recurrence Prediction Rule in a National Cohort of Veterans. Pharmacotherapy. 2018 Feb 2. doi: 10.1002/phar.2088.
- R Kaki, A Brooks, C Main, P Jayaratne, D Mertz. Does Extending Clostridium Difficile Treatment In Patients Who Are Receiving Concomitant Antibiotics Reduce The Rate Of Relapse?. The Internet Journal of Infectious Diseases. 2016 Volume 15 Number 1
- Van Hise NW, Bryant AM, Hennessey EK et al. Efficacy of Oral Vancomycin in Preventing Recurrent Clostridium difficile Infection in Patients Treated With Systemic Antimicrobial Agents. Clin Infect Dis. 2016 Sep 1;63(5):651-3
- Carignan A, Poulin S, Martin P et al. Efficacy of Secondary Prophylaxis With Vancomycin for Preventing Recurrent Clostridium difficile Infections. Am J Gastroenterol. 2016 Dec;111(12):1834-1840
- Koo HL, Koo DC, Musher DM, et al. Antimotility agents for the treatment of Clostridium difficile diarrhea and colitis. Clin Infect Dis. 2009 Mar 1;48(5):598-605
- Tiffany A. Goolsby, Bernadette Jakeman, Robert P. Gaynes, Clinical
relevance of metronidazole and peripheral neuropathy: a systematic review of the literature,
International Journal of Antimicrobial Agents (2017), http://dx.doi.org/doi:
10.1016/j.ijantimicag.2017.08.033 - Lexicomp Online®, Lexi-Drugs®, Hudson, Ohio: Lexi-Comp, Inc.; February 17, 2018.
