Chan EW, et al. Intravenous Droperidol or Olanzapine as an Adjunct to Midazolam for the Acutely Agitated Patient: A Multicenter, Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Ann Emerg Med. 2013 Jan;61(1):72-81.
Month: September 2014
Seizure Risk Associated with Tramadol Use
In an earlier post, the nuances associated the abuse potential of tramadol and its new schedule IV status, a decision made by the Drug and Enforcement Agency, was discussed. The safety of tramadol in terms of its risk for inducing seizures is a topic that is not clearly understood. Tramadol can cause seizures in overdoses because of the possible induction of serotonin syndrome and/or the modulation of monoamine reuptake inhibition. Tramadol does so by acting centrally on mu-opioid receptors and by inhibiting reuptake of serotonin and norepinephrine. Although tramadol has a weak affinity for the mu-opioid receptor, its metabolite, o-desmethyl-tramadol, has 200 times the affinity for mu-opioid receptor and is more potent in producing analgesia. Seizures have been identified as a rare complication of treatment with most opiates, but tramadol along with tapentadol and meperidine are believed to harbor the highest risk.1,2
Tramadol has been investigated as the cause of seizures on its own, but the results have been inconclusive. During post-marketing surveillance, case reports of seizures required amendment of the package insert to include a strong warning about the increased risk of seizures with therapy, especially when given concomitantly with selective serotonin re-uptake inhibitors (SSRIs), tricyclic antidepressants (TCAs), other tricyclic compounds (i.e., promethazine, cyclobenzaprine), other opioids, monoamine oxidase inhibitors (MAOIs), neuroleptics, and other drugs known to reduce the seizure threshold.3
Investigators of a large retrospective study were unable to associate tramadol use with seizures, but a small subgroup of patients with co-morbid conditions, concomitant drugs or continued treatment with tramadol may be at increased risk. It was theorized that poor metabolizers of tramadol, a polymorphism in the gene encoding CYP2D6 (present in up to 7% of Caucasians), could possibly increase the risk of seizures in patients on continued therapy.4
Another large retrospective study was conducted in order to exclude patients who had predisposing conditions to seizures to focus on the effect that tramadol might have in inducing idiopathic or newly diagnosed seizures. Comparing the differences of patients experiencing seizures receiving no analgesics, tramadol alone, other opiates alone, tramadol and other opiates or other analgesics to matched controls, the investigators observed that either taking other opiates alone or taking tramadol with other opiates was associated with an increased incidence of seizures. No patients taking tramadol alone experienced a seizure, but the calculated odds ratio for patients taking opiates alone was 5.8 (95% CI 0.6 to 51.8) and for patients taking tramadol and other opiates was 17.2 (95% CI 1.4 to 216.1) Tramadol use alone was not associated with an increased incidence of seizure.5
Yet another retrospective study attempted to investigate the risk of first time idiopathic seizures in a similar population to the previous study by Jick et al.5Investigators made it a point to evaluate cases with concomitant medications that could contribute to an increased risk of seizures. The results of this investigation were similar. For patient’s experiencing a first episode of idiopathic seizures, matched odds ratios were calculated for patient’s receiving tramadol, other opioids, tramadol plus other opioids and other analgesics. The odds ratio for patients receiving tramadol alone was 5.3 and deemed not different from matched controls (95% CI 0.6 to 48.7), but based on this information an effect could not be ruled out. For patients receiving other opioids the matched odds ratio of 8.5 (95% CI 1.3 to 56.8) and patients receiving other opioids plus tramadol the matched odds ratio of 30.6 (95% CI 2.0 to 470.8) suggest an increased incidence of seizures. In the small subset of patients taking TCAs, SSRIs and other antidepressants in addition to tramadol an increased incidence of seizures was observed.6
Although tramadol has been shown to cause seizures in the setting of an overdose, there is some evidence to show the proconvulsant effect may be dose- independent. In a study of chronic users and abusers of tramadol who experienced seizures, the mean dose between those patients who experienced seizures and those who did not were not statistically different. The most common dose range in patients that experienced a seizure was 500 to 1500 mg. This is not much higher than the maximum recommended daily dose of 400 mg. In this study population, a higher incidence of seizures was observed, occurring in nearly 46% of all patients evaluated.7
In summary, the risk of seizures in patients taking tramadol alone appears to be equal to patients not taking tramadol. However, certain risk factors may contribute to an increased risk of seizures in patients receiving tramadol. Co-morbid conditions predisposing patients to seizures, alcohol use and/or abuse, TCAs, SSRIs, MAOIs, other opiate use, other antidepressants and other drugs that may reduce the seizure threshold in conjunction with tramadol use have been associated with increased incidence of seizures. In addition, chronic users and abusers of tramadol seem to be at an increased risk of seizures.
Frank Diaz, PharmD, BCPS
Clinical Specialist, Emergency Medicine
JFK Medical Center, Edison, NJ
fdiaz64@gmail.com
Twitter: @fdiaz64
References:
- Goldfrank, L. R., & Flomenbaum, N. (2006). Goldfrank’s Toxicologic Emergencies. New York: McGraw-Hill.
- Micromedex Healthcare Series. DRUGDEX System. Greenwood Village, CO: Truven Health Analytics, 2014. http://www.thomsonhc.com/. Accessed June 14, 2014.
- Ultram [package insert]. Janssen Pharmaceuticals, Inc., Titusville, NJ; 2003. Revised 2013.
- Gardner JS, Blough D, Drinkard CR, et al. Tramadol and seizures: a surveillance study in a managed care population. Pharmacotherapy 2000; 20(12):1423-31.
- Jick H, Derby LE, Vasilakas C, et al. The Risk of Seizures Associated with Tramadol. Pharmacotherapy 1998; 18(3):607-611.
- Gasse C, Derby L, Vasilakis-Scaramozza C, et al. Incidence of first-time idiopathic seizures in users of tramadol. Pharmacotherapy 2000; 20(6):629-34.
- Talaie H, Panahandeh R, Fayaznouri M, et al. Dose-Independent Occurrence of Seizure with Tramadol. J Med Toxicol 2009; 5(2):63-67.
Emergent Treatment of Arrhythmias Associated With Wolff-Parkinson-White Syndrome
Background:
Wolff-Parkinson-White (WPW) syndrome is a congenital cardiac abnormality that manifests itself as a conduction irregularity found between the sinoatrial (SA) and atrioventricular (AV) nodes. In an otherwise healthy heart, electrical conduction begins at the SA node, which is located in the right atrium. An electrical pulse is then sent downward causing the atrium to contract and subsequently reaching the AV node, which acts as the connecting catalyst to allow the electrical pulse to reach the ventricles causing them to contract.1This pathway is controlled as electrical conduction is regulated by the SA and AV node. However, in a patient with Wolff-Parkinson-White syndrome, there is an extra pathway—also known as the accessory pathway—that allows conduction to occur directly between the atrium and ventricles, bypassing the AV node, thus leading to preexcitation of the ventricles. This preexcitation allows conduction to occur with higher and uncontrolled rates resulting in tachycardias.2 The electrocardiogram (ECG) shows a shortened PR interval and the characteristic “delta wave” which resembles a slurring slow rise of the initial portion of the QRS interval.
Pathophysiology and Treatment:
In the long-term preventative setting, WPW is managed surgically through catheter ablation.3 However, in the emergent setting treatment is dictated by specific manifestations of WPW associated arrhythmias. There is WPW with orthodromic tachycardia, WPW with antidromic tachycardia, and WPW with atrial fibrillation.4
1. WPW with orthodromic tachycardia
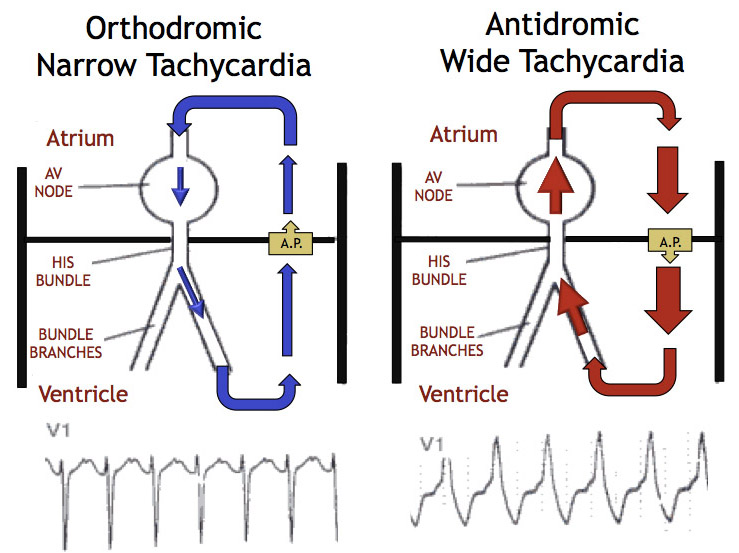
A. Orthodromic tachycardia occurs when the electrical circuit travels normally from the SA node to the AV node and down the Purkinje fibers; however, the circuit reenters the atrium via the accessory pathway causing the tachycardia as represented in Figure 1.
a. This rhythm resembles a supraventricular tachycardia (SVT) even though etiology is slightly different; however, treatment is identical.5
B. Diagnosis is made through electrocardiogram (ECG).
a. ECG will show a regular narrow QRS complex tachycardia resembling a SVT as seen in Figure 1.6
C. Treatment
a. Due to its similar mechanism as SVT, orthodromic tachycardia can be treated the same method as a SVT with an AV node blocker (AVNB).5
– Adenosine7, 8
– Verapamil8, 9
– Diltiazem8
– Beta blockers10
– Digoxin11
2. WPW with antidromic tachycardia
A. Antidromic tachycardia occurs when the electrical circuit travels from the SA node through the accessory pathway first, then up the Purkinje fibers, and through the AV node all through a retrograde or opposite direction than the orthodromic tachycardia as seen in Figure 1.
a. This rhythm resembles a ventricular tachycardia (VT), even though etiology is slightly different; however, treatment is identical.6
B. Diagnosis is also made through ECG.
a. ECG will show a regular wide QRS complex tachycardia resembling a ventricular tachycardia as seen in Figure 1.6
C. Treatment
a. It is necessary to treat with agents that selectively target the accessory pathway.
b. Procainamide
– Loading dose: 20 to 50 mg/min IV infusion until arrhythmia suppressed, hypotension ensues, QRS prolonged by 50%, or total cumulative dose of 17 mg/kg12
– Alternative loading dose: 100 mg every 5 minutes until arrhythmia is controlled or any condition described above is met.12
– Follow with a continuous infusion of 1 to 4 mg/min (must reduce maintenance dose in patients with renal impairment).12
c. Amiodarone150 mg IV over 10 minutes, then 1 mg/minute for 6 hours, then 0.5 mg/minute for 18 hours or change to oral dosing.13

Figure 1. Diagrams of orthodromic and antidromic electrical pathways and associated ECG rhythms. Available at: https://umem.org/files/uploads/content/MattuECG%20Tumblr/OrthoAnti.jpg. Accessed August 4, 2014.
3. WPW with Atrial Fibrillation
A. This is the most dangerous etiology of the WPW manifestations due to its high risk of iatrogenic error and deadly ventricular arrhythmias.2
B. In WPW with atrial fibrillation, electrical conduction in the heart travels down two paths, the normal pathway through the AV node AND from the atrium to the ventricles through the accessory pathway as seen in Figure 2.14
C. Diagnosis is made through ECG.
a. The two electrical pathways manifest themselves on ECG as irregularly irregular rhythms.
– While pulses that pass through the AV node have some rate regulation due to the AV node, impulses traveling through the accessory pathway have no rate regulation, leading to measured ventricular rates on ECG above 200 beats per minute (bpm).2
> This lack of regulation through the accessory pathway causes the irregular wave morphologies with no consistencies in the QRS waves as seen in Figure 3.
> In contrast, Figure 4 depicts a more typical atrial fibrillation without WPW where the QRS waves are seen to be more regular and ventricular rate does not exceed 150-200 bpm (due to the rate regulation caused by the AV node).
b. Atrial fibrillation with WPW is often misdiagnosed as a SVT, VT, or atrial fibrillation with a bundle branch block.
– If misdiagnosed, treatment with an AVNB will preferentially block the AV node and consequently divert all electrical impulses down the accessory pathway.15
> This shunting of electrical impulses to the accessory pathway causes ventricular fibrillation and high risk of death.
> Therefore, AVOID ALL AVNBs (i.e. adenosine, non-dihydropyridine calcium channel blockers, beta blockers, digoxin, and amiodarone) in patients with WPW with atrial fibrillation.
C. Treatment
a. Immediate cardioversionis the recommended first line treatment for hemodynamically unstable patients when WPW with atrial fibrillation presents.16
b. In a hemodynamically stable patient, procainamide can be used, as it selectively targets the accessory pathway.12
– Per 2010 ACLS guidelines, procainamide dosing is as follows:
> Loading dose: 20 to 50 mg/min IV infusion until arrhythmia suppressed, hypotension ensues, QRS prolonged by 50%, or total cumulative dose of 17 mg/kg12
> Alternative loading dose: 100 mg every 5 minutes until arrhythmia is controlled or any condition described above is met. 12
> Follow with a continuous infusion of 1 to 4 mg/min (must reduce maintenance dose for renal impairment).12

Figure 2. Diagram of WPW with atrial fibrillation with associated ECG. Available at: http://www.rjmatthewsmd.com/Definitions/supraventricular_tachyarrhythmias.htm. Accessed August 9, 2014.

Figure 3. ECG of atrial fibrillation with WPW.
Available at: http://osuemed.wordpress.com/2011/05/26/nightmare-ekg/. Accessed August 4, 2014.

Figure 4. ECG of atrial fibrillation without WPW.
Available at: http://www.emedu.org/ecg/af.htm. Accessed August 4, 2014.
3. Summary
A. WPW orthodromic tachycardias are treated as SVT with an AVNB (i.e. adenosine, verapamil, beta blockers).
B. WPW antidromic tachycardias are treated as VT with procainamide or amiodarone.
C. WPW with atrial fibrillation is treated with immediate cardioversion if hemodynamically unstable. Procainamide is a reasonable choice in hemodynamically stable patients.
Edwin Lim, PharmD Class of 2015
Thomas Jefferson University
Jefferson School of Pharmacy, Philadelphia, PA
and
Robert Pugliese, PharmD, BCPS (@theEDpharmacist)
Clinical Specialist, Emergency Medicine
Thomas Jefferson University Hospital, Philadelphia, PA
Reviewed by: Craig Cocchio, PharmD, BCPS and Nadia Awad, PharmD, BCPS
References:
1. Wolff-Parkinson-White Syndrome (WPW). Available at: http://my.clevelandclinic.org/heart/disorders/electric/wpw.aspx. Accessed July 25, 2014.
2. Sheinman BD, Evans T. Acceleration of ventricular rate by fibrillation associated with the Wolff-Parkinson-White syndrome. Br Med J (Clin Res Ed).1982;285(6347):999-1000.
3. Jackman WM, Wang XZ, Friday KJ, et al. Catheter ablation of accessory atrioventricular pathways (Wolff-Parkinson-White syndrome) by radiofrequency current. N Engl J Med. 1991;324(23):1605-11.
4. Josephson ME. Preexcitation syndromes. In: Clinical Cardiac Electrophysiology, 4th, Lippincot Williams & Wilkins, Philadelphia 2008. P.339.
5. Goy JJ, Fromer M. Antiarrhythmic treatment of atrioventricular tachycardias. J Cardiovasc Pharmacol. 1991;17 Suppl 6:S36-40.
6. Goldberger AL, Goldberger ZD, Shvilkin A. Clinical Electrocardiography: A Simplified Approach, Expert Consult: Online and Print,8, Clinical Electrocardiography: A Simplified Approach. Elsevier Health Sciences; 2012.
7. Dimarco JP, Sellers TD, Lerman BB, et al. Diagnostic and therapeutic use of adenosine in patients with supraventricular tachyarrhythmias. J Am Coll Cardiol. 1985;6(2):417-25.
8. Lim SH, Anantharaman V, Teo WS, et al. Slow infusion of calcium channel blockers compared with intravenous adenosine in the emergency treatment of supraventricular tachycardia. Resuscitation. 2009;80(5):523-8.
9. Rinkenberger RL, Prystowsky EN, Heger JJ, et al. Effects of intravenous and chronic oral verapamil administration in patients with supraventricular tachyarrhythmias. Circulation. 1980;62(5):996-1010.
10. Kowey PR, Friehling TD, Marinchak RA. Electrophysiology of beta blockers in supraventricular arrhythmias. Am J Cardiol. 1987;60(6):32D-38D.
11. Worthley LI, Holt AW. Digoxin in the critically ill patient. Crit Care Resusc. 1999;1(3):252-64.
12. Neumar RW, Otto CW, Link MS, et al. Part 8: Adult Advanced Cardiovascular Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S729-67.
13. Amiodarone Package Insert. Available at: http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=cdd50dc7-f712-4248-b0e3-ba247cf08cee#cbb97eba-08e3-4a99-ac87-e4697427b866. Accessed August 22, 2014.
14. Das MK, Zipes DP. Electrocardiography of Arrhythmias, A Comprehensive Review. Elsevier Health Sciences; 2012.
15. Schützenberger W, Leisch F, Gmeiner R. Enhanced accessory pathway conduction following intravenous amiodarone in atrial fibrillation. A case report. Int J Cardiol. 1987;16(1):93-5
16. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2014.

{kind=link}
You must be logged in to post a comment.