A new blog post I wrote on the HYMR Blog!
A new blog post I wrote on the HYMR Blog!
A
The Gist:
As an Emergency Medicine Pharmacist (EMP), I think of toxicology as trauma at the cellular level.
An acute isoniazid (INH) poisoning causes seizures that may be refractory to benzodiazepines. An acute INH ingestion of 80 – 150 mg/kg is associated with increased mortality.[2] In addition to seizures, INH poisoning can cause vomiting, coma, tachycardia, renal failure, lactic acidosis, profound anion gap metabolic acidosis, liver injury, and hypotension.
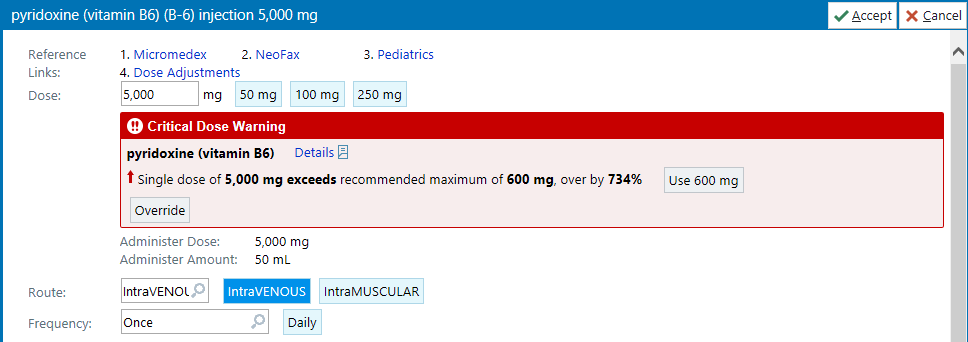
PYRIDOXINE (vitamin B6) 5 grams IV is the specific antidote, dose, and route to terminate seizures if the amount of INH ingestion is unknown.[1-3]
Pyridoxine is an essential cofactor to make gamma-aminobutyric acid (GABA), the primary inhibitory neurotransmitter in the CNS. INH interferes with pyridoxine metabolism, resulting in a GABA deficit. The depletion of GABA leads to uninhibited electric activity resulting in seizures. This also explains why INH poisonings can be refractory to benzodiazepines. Recall that benzos modulate the GABA receptor to enhance the effect of GABA but the problem is, the CNS now has a GABA deficit, so there is little GABA to bind. This is why a large dose of pyridoxine can overcome an INH poisoning and swing the metabolic pendulum to restoring GABA production and ultimately terminate seizures.[1-3]
The Story:
There is always a story when you administer a critical drug in real life.
The purpose of this post is to shed light on how a drug therapy recommendation was conceived and how it manifests into the last drop flowing into the patient’s vein when it mattered most. I have been a pharmacist for twelve years now, the last six specializing in emergency medicine. Over the years, from practicing and striving to stay current, with respect to treating an INH overdose, I just filed it away in my mental catalogue thinking, “That’s cool, makes a good toxicology test question but I’ll likely never treat one.” It mentally lives alongside random tox info like remembering the one time in residency I assisted giving methylene blue 2 mg/kg IV to a young man who developed topical benzocaine-induced methemoglobinemia after an ENT procedure. You just think, “I’m not ever going to use this stuff” or “I’ll likely never see that again”. My advice: Be ready. You might encounter a similar case on your next shift. I feel inclined to share what unfolded and illustrate some roles of an EMP. I’m unable to find a detailed eyewitness account from an EMP perspective regarding what actually happened during an INH poisoning when pyridoxine IV was given. Here’s mine.
The year is 2013 and I stumbled upon this blog. I recall reading Nadia Awad’s May post on pyridoxine for refractory status epilepticus that highlighted a serious issue where hospitals either did not stock pyridoxine IV or had inadequate stock. I recently began my EMP career, and this motivated me to check our stock. I found out we also had inadequate stock. I immediately discussed this with our Pharmacy Buyer and Lead Pharmacy Tech in charge of our automated vertical storage system to update our pyridoxine inventory to a minimum of 50 vials and a max of 100 vials. Our wholesaler only has pyridoxine 100 mg/mL x 1 mL vials (25/pack) available. It has good shelf life and costs less than $300 for a life-saving 5 gram IV dose. I ensured it was in stock since then and knew exactly where it lived in the pharmacy.
The Case:
Prior to ED arrival, EMS reports adult female with seizures. ED blast page “Code 3 Ambulance has arrived to room 32”. That’s our isolation room. Our ED cavalry descends on the room, we all turn the corner and see four EMS/Fire crew members wearing N95s with a young female on the gurney appearing comatose with a nasal pharyngeal airway in. After attending FEMA’s Center for Domestic Preparedness Healthcare Leadership for MCI course- it’s now engrained in me to “Protect this House.” Don’t dither, question anything that might pose a threat to staff and patients inside. I immediately asked out loud, “Whoa! HOLD ON. Why the N95s?” EMS replies, “We were told she has TB.” For a second, it felt like an Oprah moment with the team handing out masks, “You get a N95. You get a N95…” (after resuscitation we later confirmed the patient had latent TB, which is not contagious).
In a fraction of a second, I remember thinking—“Oh my gosh, seizures, TB…did she overdose on INH? We might need vitamin B6!”
EMS reports the 29 year-old-woman with history of depression intentionally overdosed on her INH to harm herself. She was drinking a beer with her significant other when she told him that earlier she had looked up the side effects of INH on her phone and took too many. She then handed her phone over to show him the side effects of an INH overdose. Shortly after, she became weak and had a witnessed seizure. During EMS transport, she had 3 more seizures. Midazolam 2 mg IV was given en route with estimated time of ingestion, maybe 2 hours ago. She presents with sinus tach, BP 98/54, temp 36.4 C (axillary), RR 20, SpO2 96%, blood sugar 166, weighing 45 kg, obtunded, postical, weak moans and withdrawals to painful stimuli in all 4 extremities. EMS states she only takes two medications and holds up the bottles. I checked the labels—one is a pretty full bottle of pyridoxine 50 mg tablets #30, recent fill, confirmed the tablets inside were pyridoxine 50 mg and saw the other labeled bottle for isoniazid 300 mg #30 tablets. The bottle was empty. However, even though the quantity shows 30 tablets, there could have been other bottles at home, stocked up refills, or there could have been a medley of oral medications in this bottle from who knows where. Later, we found out the patient had a tendency to store new INH prescriptions in various amounts in old bottles. So, I didn’t get to play one of my favorite ED games – Guess That Pill. (My other favorite games include Guess that ETOH level, or pretending to be a professional carnival weight guesser). In my head I was thinking, “Well this could be a polypharmacy ingestion but she’s absolutely getting B6. I’ve always read about this, I’ve never done this and don’t know what will happen after I give it but this is going to happen.” I’ll admit, I was excited to help her and put some knowledge to work.
Right after the patient moved to our gurney, she had a generalized tonic-clonic seizure that lasted for less than 1 minute.
I recall RNs verbalizing recommendations to give lorazepam, levetiracetam, or prep for intubation. At that moment, based on what I was hearing, I felt like I had the key answer to really help this patient so I told the team in a calm but loud voice “Give Ativan but the life saving antidote for an INH overdose is vitamin B6 IV. It is in the main pharmacy. I’m going to get it.”
The ED Physician said, “OK, what’s the dose and how fast can you get it here?” I replied, “5 grams. Give me 10-15 minutes.”
The ED doc assessed her airway and decided to monitor closely and not intubate at that time.
Getting The Pyridoxine:
For me, part of the magic and benefit of being an EMP is making a drug recommendation physically happen quickly and safely. This also involves deciding where the drug is stored, ensuring adequate quantities are on hand, optimizing how it’s ordered in the EHR, documenting recommendations for the inpatient team, preparing the drug, and relaying how to safely and appropriately administer the drug.
I turned around and called an inpatient pharmacy tech. Paraphrasing, I told her calmly and directly, “Please listen to me carefully. Stop whatever you are doing. There is a woman in the ED who needs a life saving drug now. Go to the MedCarousel, take out 50 vials of pyridoxine 1 mL vials and give it to the IV tech. Have the tech straight draw the 50 mL undiluted and shoot it all into a Viaflex bag. A label will print out in just a minute. I’m coming down now.”
I figured the IV room tech could draw it up by the time I could get there (sterile too) since main pharmacy is in the basement on the other side of the hospital. Nevertheless, if I had vials in the ED, I have no qualms about drawing it up in the ED medication room or at bedside for such an emergent indication even though my IV room/sterile compounding colleagues might cringe at that idea. My ED folks get it.
**Note: if I had to treat another INH poisoning, I would straight draw the 50 vials into a 60 mL syringe. I would give the pyridoxine undiluted IV push because we can control rate of administration and given it’s a relatively small volume, eliminate concern for residual drug in the IV tubing which would underdose the patient. I have no data to back up this IV push undiluted recommendation aside from drug info stating to administer at rate of 1 g/min (i.e., 5 minutes) and my one experience where 5 g was given IV undiluted over 1-2 minutes via a 16G peripheral AC line without any local or vital sign ADRs.**
EHR Issues:
I login to our EHR, input the order for 5,000 mg and a warning box screams back at me with not 1 but 2 shades of red with double exclamation points. Even though I was confident in the dose, in that moment, reflexively I thought, “WARNING. STOP. Backup. Do not pass GO and collect $200.” I double-checked that I selected the correct drug, dose, product and then accepted. Mental note: I’ll have to work with IT later and add verbiage to this orderable about pyridoxine dosing and administration for INH overdose so in future the person ordering can feel confident and safe hitting accept and prevent any delays.

To The Pharmacy:
I clicked verify, tapped my badge to logout from the ED computer, called California Poison Control (CPC) to open a case from the ED Pharmacist “bat phone” as I made a beeline to the main pharmacy.
CPC gave me some more tox info and stated that if the patient seizes again after first dose of pyridoxine then repeat another 5 gram IV dose.
When I got down to the pharmacy, the IV tech already had the labeled bag and empty vials ready for me outside the pass through window. I counted the 50 vials, nothing expired and all were correct, then jetted back to the ED.
Let It Flow:
Right when I stepped back into the ED, holding the IV bag, my phone rang. CPC Pharmacist called back recommending to dilute the pyridoxine in 50 mL of NS or D5W and infuse over 5 minutes.[3] A second later, ED Code Blue alarm goes off. I asked the Lead Clerk, “What room?”. She replied, “Room 32”. I said “Oh $#!t. That’s the girl. I’ll call you back.” CPC Pharmacist replied, “No problem, do your thing.”
In the 6 seconds it took me to walk to the room, I am thinking- I have this potentially life saving magical liquid sloshing around in this bag. I’m not going to draw out the 50 mL and push it into another bag and dilute it. I cannot recall seeing or learning any information that B6 IV will cause extravasation. This also is not going on a smart pump either, real concern for residual in distal portion from the pump cassette and waste of precious minutes to set up as a secondary.
The patient is seizing for the 6th time and the ED team is now at bedside. Told the doc I have the pyridoxine and got a head nod to give it. I grabbed primary roller clamp tubing, primed the line, and handed it to the RN who stands 6 ft 4in. He asks, “Ravi, how fast?”. I replied, “Let it rip!” He did the Statue of Liberty pose, his arm height higher than any IV pole and used his hand like a pressure bag to squeeze the bag. We followed every last drop down to the extension set needle-free connector. The 50 mL volume infused over 60 to 120 seconds. There were no ADRs seen with drug administration with respect to negative impact on HR, BP, RR, O2, or IV site. It took about 20 minutes from when EMS gurney entered our ED to the last drop of pyridoxine flowing into the vein. When it was all in, she immediately stopped seizing. Was it the pyridoxine or did the seizure just stop? We’ll never know, but what we do know is that after the pyridoxine, the patient never seized again throughout the hospitalization. We followed up with lorazepam 1 mg IV. Over the course of an hour, she became more awake, moving in bed, moaning and groaning, mental status improving, vomited once and was able to keep her eyes open and look around.
I made an EHR note documenting CPC information detailing INH toxicity, treatment, and recommendation for a 2nd dose of pyridoxone 5 grams IV if patient seizes again. This note was important because all subsequent physician specialists referred to this note and incorporated it into their notes.
Results:
Patient had a profound anion gap metabolic acidosis. Recall the “I” in the mnemonic MUDPILES, refers to INH and is used to remember causes of increased anion gap metabolic acidosis.
Initial results remarkable for: lactate 19; anion gap 31; bicarb 6, K 2.9; Scr 1.10 (baseline 0.49). 12-lead ECG revealed prolonged QTc 570 ms. Urine drug screen, APAP, ASA levels all negative. LFTs WNL. Alcohol 0.092. Patient was initially resuscitated with NS x 2L, mag sulfate 2 gram IV, bicarb 50 meq, and potassium repletion. About 2.5 hours post fluid bolus, repeat lactate was 5.5. Repeat anion gap was 11, seven hours post pyridoxine administration.


I checked main pharmacy inventory again, we had 50 vials of pyridoxine 100 mg/mL x 1 mL remaining. Before I went home, I signed out with our main pharmacy night pharmacist. I verbally conveyed the inventory on hand, its location in the pharmacy, to ignore the EHR critical dose warning, how to administer another dose, and requested Rx tech to order 50 more vials.
The patient was admitted to the ICU for monitoring. She had no subsequent seizures. Aside from the midazolam 2 mg IV given by EMS, single pyridoxine 5 gram IV and lorazepam 1mg IV dose given in ED no other seizure medications were given nor required during the remaining hospitalization. The patient had a full recovery and was discharged to Behavioral Health 2.5 days later given the suicide attempt.
Just prior to discharge I went up to the ICU to speak with her and she revealed that she took 14 INH 300 mg tablets (4.2 grams of INH; weight = 45 kg; dose = 93 mg/kg = potentially lethal dose).
Inventory Recheck:
Work is never done. Just the other day, I randomly checked our pyridoxine inventory and saw that the par level min and max were now min 15 max 25. We had 100 vials on hand. I worked with our Lead Rx tech to update our min and max to 100. It reinforces the fact that it’s important to randomly verify your antidote par levels a few times a year to avoid waste but also to ensure par wasn’t reduced accidently or was not reordered.
Finding Purpose:
When the dust had settled, I made it a point to say thank you face-to-face and express gratitude to the inpatient Rx tech, IV tech, our Rx buyer, and Lead Pyxis tech for helping to ensure the med was available, all systems worked as they designed, and that the med was quickly and safely prepared. I shared with them details of just how critical this drug was and how their concerted efforts played a vital role in saving this woman’s life. I firmly believe it’s important to reinforce that their work has real purpose. Our pharmacy techs work hard and are highly skilled but don’t always hear about what goes on upstairs and the positive results from their work. I’m always grateful for their skill and dedication.
A colleague reminded me of a President John F. Kennedy story. In 1962, JFK visited NASA space center for the first time. During his tour, he met a janitor carrying a broom down the hall and JFK asked him what he did for NASA. The janitor replied, “I’m helping put a man on the moon.” We all play a part in something phenomenal. Empower your colleagues with purpose and show gratitude. One goal I strive for is that if you ask our pharmacy techs what they do, I hope they reply with a smile, pride, and a sense of purpose, “I help save lives.”
Ravi Singh, Pharm.D.
Emergency Medicine Pharmacist
John Muir Health – Walnut Creek Medical Center
Walnut Creek, CA
Twitter: @RaviEMPharmD
References:
Ref – This post is largely based on an amazing review article by one of the most brilliant physicians ever: Chiral Toxicology: It’s the Same Thing…Only Different
Some believe there is a departure from basic chemistry after entering professional pharmacy education. However, encountering numerous drugs in clinical practice, we knowingly focus on clinical properties, clinical evidence, and collaborative efforts with the treatment team.
Chemical principles like isomers are one of these elements we tend to leave behind. We may have tossed the term around clinically lately, but recalling the basic chemistry and subsequent pharmacology is interesting. Although they share the same molecular formula, isomers are chemical structures with different structural formulas. This can translate into entirely different chemical properties. One example is the constitutional or structural isomers with the molecular formula C7H8O that, for example, can be benzyl alcohol (phenyl methanol) or methoxybenzene. They have completely different physical properties but the same molecular weight and formula.

Stereoisomers can be further split into configurational isomers or conformational isomers. Configurational isomers are differed based on their structural rotation when looking down based on a Newman projection. When the optical arrangement is made where the main groups are 180 degrees from each other, it is called the anti-staggered rotation. When the main groups are 60 degrees rotated, they’re now in the gauche arrangement; with 120 degrees, they’re eclipsed, and at zero degrees, they’re totally eclipsed.

The other main conformational isomer idea is the cyclical conformation of the ring structure. The chair cyclohexane is familiar and is the most stable formation for many.
Configurational isomers, on the other hand (funny since we can use our hands as examples of chiral structures), are broken into two large groups, enantiomers and diastereomers. We’re familiar with these concepts if we know drug names, such as albuterol and levalbuterol.
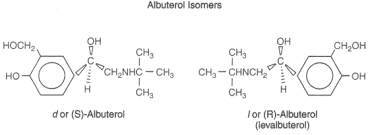
Albuterol and levalbuterol are identical molecular formula compounds but differ in a three-dimensional arrangement. The chiral carbon on the albuterol structure has an S configuration, whereas, in levalbuterol, it is in the R- configuration. This may not seem obvious since doesn’t “lev” stand for L? In many cases, yes, but in this case, it’s inaccurate based on our modern understanding of these structural relationships. The D (dextrorotatory, or -) and L (levorotatory, or +) are somewhat different in how they’re identified compared to R (rectus) and S (sinister). That is related to the D and L enantiomers are determined based on the structure’s rotation of polarized light. Rotation to the right (clockwise) indicates a D or – characteristic, whereas the L is to the left (or counterclockwise). An example of when this doesn’t correlate accordingly is with albuterol and levalbuterol. Albuterol has an S configuration at its chiral center, whereas levoalbuterol has an R configuration. So one could wrongly assume levalbuterol has an “S” or to the Left confirmation when it’s to the right. However, numerous drugs align with this, including levofloxacin (L or S – ofloxacin) or escitalopram (L or S – citalopram).
Another structural description includes the cis- and trans-conformation compared to the Z- (zusammen) and E- (entgegen) diastereomers. The cis-trans isomers have their highest priority substituents on the particular side of the bond. Cis- has its substituents on the same side of immovable bonds, whereas the trans has these groups on either side of the immovable bonds. However, when the compound has polysubstituted double bonds, this doesn’t work. We can use the E/Z designation from the Cahn-Ingold-Prelog priority (also established R/S). For Z- the two highest priority groups are on the same side of the double bond, whereas E is on opposite sides. An example of where these can differ includes looking at cisatracurium-atracurium and tretinoin-isotretinoin. The cis is based on two chiral Nitrogens (not carbon) and two chiral carbons with cisatracurium. Conversely, tretinoin has four E- conformations, whereas isotretinoin has three E- and one Z conformations.




You must be logged in to post a comment.