Many institutions have implemented antimicrobial restriction programs where specific agents, based on toxicity, cost, or broad-spectrum of activity, require special permission for use. Often a page is required to initiate the request. During my infectious diseases PGY-2 I carried this antimicrobial approval pager, either approving the use of restricted agents or offering suggesting on alternative therapy. Fluoroquinolones (FQs) were by far, the most requested restricted antimicrobials, and also the most denied. In emergency departments without such programs, pharmacists play a vital role in antimicrobial stewardship, steering therapy to optimize clinical outcomes while minimizing unintended consequences. With their broad spectrum of activity, oral formulation, and seemingly minimal adverse effect profile, FQs were highly touted when originally approved. However, after decades of clinical use and research, is it time we rethink their greatness?
The most commonly reported side effects of FQs are what you will see as the most common side effects for just about every drug out there: nausea, vomiting, and diarrhea. Where FQs really separate themselves is the frequency and variety of severe safety issues they have been associated with, including but not limited to the following:
|
Commonly Known Adverse Effects
|
Lesser Known Adverse Effects
|
|
QT prolongation
|
GI perforation
|
|
Clostridium difficile infection
|
Aortic aneurysm/dissection
|
|
Tendinopathy
|
Retinal detachment
|
|
Peripheral neuropathy
|
Hypo/hyperglycemia
|
|
Black box warnings
|
Seizures/Psychiatric AEs
|
-
QT prolongation- FQs prolong the QT interval in a dose dependent fashion by blocking voltage-gated potassium channels.1 A rare but potentially fatal consequence is torsades de pointes.2 A retrospective review of patients experiencing torsades de pointes associated with the administration of a FQ found that 96% of patients had at least one additional risk factor.3 These included electrolyte abnormalities, concurrent use of a QT-prolonging medication, prolonged QT interval at baseline, cardiovascular disease, bradycardia, and female sex.
-
Clostridium difficile Infection (CDI)- The most important modifiable risk factor for CDI is exposure to antimicrobial agents. While exposure to just about every antibiotic has been associated with CDI, more broad spectrum agents generally place patients at a higher risk. A retrospective study conducted over an 18 month period found FQs as the antibiotic class most strongly associated with CDI (Adjusted HR, 3.44; 95% CI, 2.65–4.47).4 The next highest class, 2nd generation cephalosporins, was almost half of FQs (Adjusted HR, 1.89; 95% CI, 1.45-2.46). Furthermore, an interrupted time-series analysis evaluating CDI pre- and post-implementation of a FQ restriction program found a reduction in FQ usage was associated with a reduction in CDI cases (rate ratio: 0.332; 95% CI: 0.240-0.460).5
-
Seizure- Certain FQs lower the seizure threshold by displacing GABA or competing with GABA binding at receptor sites within the central nervous system (CNS).6 While the overall risk of serious CNS reactions is low, it is likely more pertinent in susceptible patients, such as those with underlying CNS disorders, such as epilepsy, cerebral trauma, or anoxia.7,8 Furthermore, concomitant NSAID use increases the risk of seizures with FQs.9
-
Peripheral Neuropathy- Beginning August 2013, the Food and Drug Administration (FDA) required FQs to carry a black box warning regarding peripheral neuropathies.10,11,12 A case-control study of male subjects concluded the risk of peripheral neuropathy was doubled in patients newly taking FQs (RR = 2.07, 95% CI 1.56-2.74).13 A finding that becomes more troubling when taking into account case reports describing that these neuropathies may be irreversible.14
- Psychiatric Adverse Reactions- The CNS effects of FQs can also include mental health adverse reactions. A potential mechanism for this is FQ induced decreases in brain serotonin and GABA levels,26 In July 2018, the FDA strengthened current warnings in the prescribing information to include that FQ antibiotics may cause significant mental health side effects; Recommending that clinicians inform patients about the risk of psychiatric adverse reactions that can occur after just one dose.25
-
Glucose abnormalities- The package inserts for ciprofloxacin, levofloxacin and moxifloxacin all warn of the possibility of both hypoglycemia and hyperglycemia.10,11,12 Hypoglycemia is explained by the ability of FQs to close K+-ATP channels in pancreatic islet cells causing the release of insulin.15 The mechanism leading to hyperglycemia is not well understood. Patients with diabetes are at the highest risk of experiencing glucose abnormalities. Chou et al conducted a population-based inception cohort study with 78,433 diabetic patients enrolled in order to evaluate the risk of dysglycemia among patients receiving levofloxacin, ciprofloxacin, moxifloxacin, cephalosporins, and macrolides.15 The absolute risk of hyperglycemia per 1000 persons was found to be 1.6 for macrolides, 2.1 for cephalosporins, 3.9 for levofloxacin, 4.0 for ciprofloxacin, and 6.9 for moxifloxacin. The absolute risk of hypoglycemia was found to be 3.2 for cephalosporins, 3.7 for macrolides, 7.9 for ciprofloxacin, 9.3 for levofloxacin, and 10.0 for moxifloxacin. In July 2018, the FDA strengthened the the current warnings in the prescribing information that FQ antibiotics may cause significant decreases in blood sugar; Suggesting that clinicians should alert patients of the symptoms of hypoglycemia and carefully monitor blood glucose levels in patients receiving FQs.25
-
Gastrointestinal (GI) Perforation- FQs can reduce the expression and size of type I collagen fibrils causing deleterious effects on collagen and connective tissues.16 This is the likely mechanism behind FQs increased risk of GI perforation, and many of the adverse events listed below (tendinopathy, retinal detachment and aortic dissection/aneurysm). A nested case control study conducted over a 13 year year period found that current use of a FQ was associated with an increased risk of GI perforation (RR, 2.16; 95% CI, 1.85±2.53).17 The increase in risk of GI perforation remained even after adjusting for disease risk score (RR, 1.90; 95% CI, 1.62-2.22) and disease risk score matching (RR, 1.88; 95% CI, 1.44 -2.46).
-
Tendinopathy- Since July 2008, the FDA has required FQs have a black-box warning regarding adverse events, specifically citing tendonitis and tendon rupture. In a large population-based case control analysis, patients taking FQs were 4.1 times more likely to experience achilles tendon rupture than control patients.18 Elderly patients, and patients taking concurrent corticosteroids appear to be at an even higher risk of tendinopathy. In fact, the author’s determined the concomitant use of corticosteroids and FQs increased the risk of achilles tendon rupture 43.2-fold.
-
Retinal detachment- While a rare occurrence in general, FQ use has been associated with an increased risk of retinal detachment. A nested case-control study, with 4,384 cases of retinal detachment and 43,840 controls, found current use of FQs was associated with a significantly higher risk of developing a retinal detachment (adjusted RR, 4.50, 95% CI, 3.56-5.70).19 Additionally, a case-crossover study including 27,540 patients found a 1.46-fold increased risk for retinal detachment during the 10-day period after the dispensing of oral FQs.20
-
Aortic dissection/aneurysm- In another nested case-control analysis, after propensity score adjustment, current use of FQs was found to be associated with increased risk for aortic aneurysm or dissection (rate ratio, 2.43; 95% CI, 1.83-3.22).21
-
Black box warnings- As previously mentioned, FQs have a black box warning regarding tendinopathy and peripheral neuropathy. They also carry a black box warning for use in patients myasthenia gravis as they may exacerbate muscle weakness. Additionally, in May of 2016 the FDA added that due to safety concerns, FQs should be reserved for patients with no other treatment options for acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, and uncomplicated urinary tract infections.
-
Drug-drug interactions- In addition to additive QT prolongation with other QT prolonging medications and increased risk of tendinopathy with corticosteroids, ciprofloxacin is a CYP1A2 inhibitor. This property is of particular importance when considering the interaction between ciprofloxacin and tizanidine which increases the area under the curve (AUC) of tizanidine 10-fold, leading to an increased risk of hypotension and extreme sedation.22
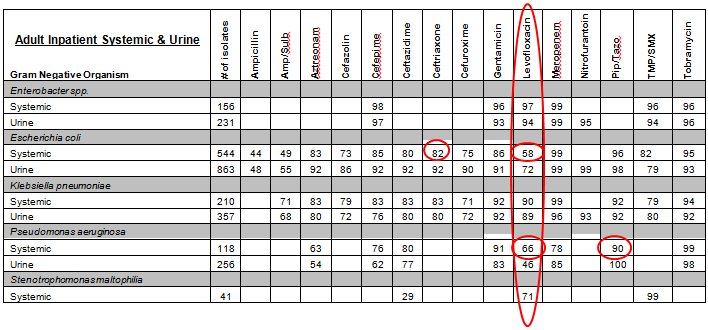
If the above list of adverse effects wasn’t convincing enough, there is an entirely different aspect to be concerned about, resistance. FQ resistance has grown rapidly since their invention.23 Part of the rapid emergence is due to a low barrier to resistance. A single mutation in the bacterial topoisomerase gene can confer high-level resistance.24 A great way to get an idea of FQ susceptibilities specific to your patient population is to look at your institution’s antibiogram. Below is a real antibiogram. Notice levofloxacin isn’t the best option against any pathogen listed when it comes to in-vitro susceptibility. For example, systemic E.coli and Pseudomonas aeruginosa susceptibilities to levofloxacin are only 58% and 66%, respectively! Compare that with 82% susceptibility of E.coli to 3rd generation cephalosporins and 90% susceptibility to this institution’s antipseudomonal work-horse, piperacillin-tazobactam, and you’ll get an idea of just how inferior FQs can be empirically. Take a look at your own antibiogram, I’d be willing to bet it looks similar. Feel free to share in the comments.
With all of the negative information presented above, one might be asking exactly when, or if FQs should be used? While FQs should rarely be the first choice antibiotic, I believe there is a role for them in emergency medicine, and when making recommendations I tend to use them in a few scenarios. The first scenario is to provide gram-negative coverage in patients with true IgE-mediated beta-lactam allergies. Situations like these underscore how important it is to clarify allergies so that only patients who cannot safely receive a beta-lactam are being given less active therapy, like FQs. Another situation in which I use FQs may be when monotherapy is preferred due to patients specific factors, such as cost or compliance, for a condition that may require multiple antibiotics otherwise (ie community acquired pneumonia- levaquin vs 2nd/3rd gen cephalosporin + azithromycin). Next, acknowledging it is a clinical controversy, if faced with a situation in which we must treat a gram-negative bacteremia with oral therapy, I always reach for a FQ given their high level of oral bioavailability. Lastly, I recommend FQs in any situation where a Pseudomonas spp. has been isolated, or there is strong suspicion of it, and oral therapy is desired. This highlights another great reason to use FQs sparingly; ciprofloxacin and levofloxacin are our only reliable oral antipseudomonal agents, overuse could compromise this activity and leave us in a situation where all Pseudomonas spp. infections would require intravenous therapy.
FQs are no longer the catch-all antibiotic they were once thought to be. Resistance rates have increased rapidly while a laundry list of severe safety issues have come to light. We are now in an era where both the safety and the efficacy of FQs is questionable, at best. It’s time we start utilizing them that way.
Take Home Points
-
FQs have been associated with many severe adverse reactions, including but not limited to QT prolongation, CDI, seizures, peripheral neuropathy, psychiatric issues, hypo/hyper glycemia, GI perforation, tendinopathy, retinal detachment, aortic dissection/aneurysm, as well as causing drug-drug interactions.
-
FQs carry multiple black box warnings surrounding their safety.
-
FQs have a low barrier to resistance.
-
Resistance rates to FQs have increased rapidly. Look at your antibiogram!
-
Ciprofloxacin and levofloxacin are our only oral agents with reliable activity against Pseudomonas spp.
-
FQs should be reserved for a few clinical scenarios where other antibiotics are not safe or feasible.
Tony Mixon, PharmD, BCPS
Emergency Medicine/Infectious Disease Clinical Pharmacist
University of Colorado Health- North Region
Peer reviewed by Craig Cocchio, PharmD, BCPS (@iEMPharmD) and Nadia Awad, PharmD, BCPS (@Nadia_EMPharmD)
References:
-
Briasoulis A. Agarwal V. Pierce W.J. QT prolongation and torsade de pointes induced by fluoroquinolones: infrequent side effects from commonly used medications. Cardiology. 2011;120(2):103-10.
-
Mehrzad R, Barza M. Weighing the adverse cardiac effects of fluoroquinolones: A risk perspective. J Clin Pharmacol. 2015 Nov;55(11):1198-206
-
Zeltser D, Justo D, Halkin A, Prokhorov V, Heller K, Viskin S. Torsade de pointes due to noncardiac drugs: most patients have easily identifiable risk factors. Medicine. 2003; 82:282–290
-
Pépin J, Saheb N, Coulombe MA, et al. Emergence of fluoroquinolones as the predominant risk factor for Clostridium difficile-associated diarrhea: a cohort study during an epidemic in Quebec. Clin Infect Dis. 2005 Nov 1;41(9):1254-60
-
Sarma JB,, Marshall B, Cleeve V. Effects of fluoroquinolone restriction (from 2007 to 2012) on Clostridium difficile infections: interrupted time-series analysis. J Hosp Infect. 2015 Sep;91(1):74-80
-
Domagala JM. Structure-activity and structure-side-effect relationships for the quinolone antibacterials, J Antimicrob Chemother , 1994, vol. 33 (pg. 685-706)
-
Christ W, Central nervous system toxicity of quinolones: human and animal findings. J Antimicrob Chemother. 1990 Oct;26 Suppl B:219-25
-
Owens RC Jr, Ambrose PG. Clinical use of the fluoroquinolones, Med Clin N Am , 2000, vol. 84 (pg. 1447-69)
-
Akahane K, Kimura Y, Tsutomi Y, et al. Possible intermolecular interaction between quinolones and biphenylacetic acid inhibits gamma-aminobutyric acid receptor sites. Antimicrob Agents Chemother. 1994 Oct;38(10):2323-9.
-
Product Information: CIPRO(R) IV injection, ciprofloxacin IV injection. Bayer HealthCare Pharmaceuticals, Inc. (per FDA), Montville, NJ, 2011.
-
Product Information: LEVAQUIN(R) oral film coated tablets, solution, intravenous injection solution, levofloxacin oral film coated tablets, solution, intravenous injection solution. Janssen Pharmaceuticals, Inc. (per FDA), Titusville, NJ, 2016.
-
Product Information: AVELOX(R) oral tablets, intravenous injection, moxifloxacin HCl oral tablets, intravenous injection. Bayer HealthCare Pharmaceuticals Inc. (per manufacturer), Whitehouse Station, NJ, 2015.
-
Etminan M, Brophy JM, Samii A. Oral fluoroquinolone use and risk of peripheral neuropathy: a pharmacoepidemiologic study. Neurology. 2014 Sep 30;83(14):1261-3.
-
Francis JK, Higgins E. Permanent Peripheral Neuropathy: A Case Report on a Rare but Serious Debilitating Side-Effect of Fluoroquinolone Administration. J Investig Med High Impact Case Rep. 2014 Jul 27;2(3)
-
Chou HW, Wang JL, Chang CH et al. Risk of severe dysglycemia among diabetic patients receiving levofloxacin, ciprofloxacin, or moxifloxacin in Taiwan. Clin Infect Dis. 2013 Oct;57(7):971-80.
-
Tsai WC, Hsu CC, Chen CP, Chang HN, Wong AM, Lin MS, et al. Ciprofloxacin up-regulates tendon
cells to express matrix metalloproteinase-2 with degradation of type I collagen. Journal of orthopaedic
research: official publication of the Orthopaedic Research Society. 2011; 29(1):67±73 -
Hsu SC, Chang SS, Lee MG et al. Risk of gastrointestinal perforation in patients taking oral fluoroquinolone therapy: An analysis of nationally representative cohort. PLoS One. 2017 Sep 5;12(9):e0183813
-
Corrao G, Zambon A, Bertù L. Evidence of tendinitis provoked by fluoroquinolone treatment: a case-control study. Drug Saf. 2006;29(10):889-96.
-
Etminan M, Forooghian F, Brophy JM et al. Oral fluoroquinolones and the risk of retinal detachment. JAMA. 2012 Apr 4;307(13):1414-9.
-
Raguideau F, Lemaitre M, Dray-Spira R et al. Association Between Oral Fluoroquinolone Use and Retinal Detachment. JAMA Ophthalmol. 2016 Apr;134(4):415-21.
-
Lee CC, Lee MT, Chen YS et al. Risk of Aortic Dissection and Aortic Aneurysm in Patients Taking Oral Fluoroquinolone. JAMA Intern Med. 2015 Nov;175(11):1839-47
-
Granfors MT, Backman JT, Neuvonen M et al. Ciprofloxacin greatly increases concentrations and hypotensive effect of tizanidine by inhibiting its cytochrome P450 1A2-mediated presystemic metabolism. Clin Pharmacol Ther. 2004 Dec;76(6):598-606
-
Jacoby GA. Mechanisms of resistance to quinolones. Clin Infect Dis. 2005 Jul 15;41 Suppl 2:S120-6
-
Redgrave LS, Sutton SB, Webber MA et al. Fluoroquinolone resistance: mechanisms, impact on bacteria, and role in evolutionary success.Trends Microbiol. 2014 Aug;22(8):438-45.
- https://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm612979.htm
- Ilgin S, Can OD2, Atli O. Ciprofloxacin-induced neurotoxicity: evaluation of possible underlying mechanisms. Toxicol Mech Methods. 2015;25(5):374-81
