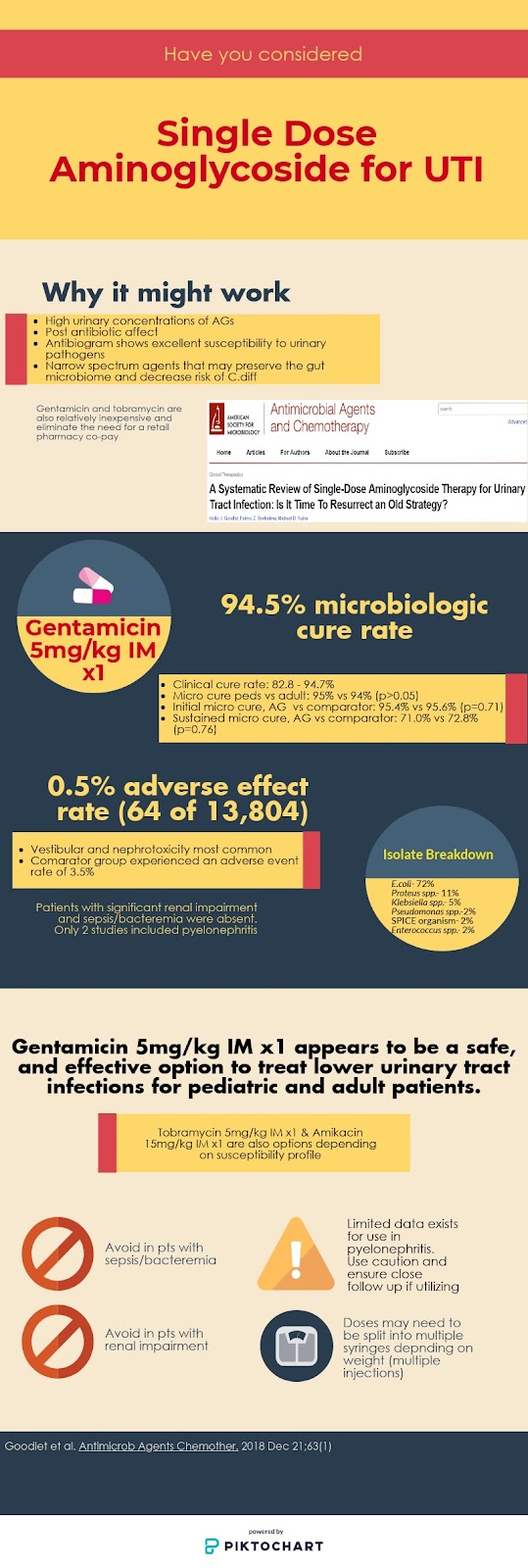
Looking for a single dose, no compliance issues, inexpensive, safe, and effective option to treat urinary tract infections? An older therapeutic option might be the answer. A recent systematic review by Goodlet et al. looks into the utility of single dose aminoglycosides (AGs) to treat cysitis.1
Kellie J. Goodlet, PharmD , Fatima Z. Benhalima, and Michael D. Nailor, PharmD
Design
Systematic review conducted in accordance with PRISMA guidelines, and of original research studies published in the english language meeting the following inclusion criteria:
Use of an AG as a single dose therapy
No concomitant antibiotic therapy
Indication = UTI
Evaluation of microbiologic and/or clinical cure
Excluded:
Unpublished studies
Conference abstracts
Gray literature
Outcomes Investigated
Microbiologic cure- documented eradication of bacteria from the urine within 7 days of antibiotics
Clinical cure- resolution of UTI symptoms
Reinfection- UTI recurrence on days 15-30 after antibiotics and/or different infecting organism from initial infection
Relapse- UTI recurrence on days 1-14 after antibiotics
Results
13 articles representing 13,804 patients met inclusion criteria
All were published between 1978-1991
7 studies had comparator arms consisting of one of the following:
1 study including moderate-severe renal dysfunction with a total of 10 patients falling into these categories
Type of UTI
6 studies only included lower UTI
2 studies included patients with pyelonephritis
5 studies did not report type of UTI
Sepsis/Bacteremia
No cases reported in these studies
Intervention
Gentamicin 3-5 mg/kg intramuscularly used in 3 studies
Amikacin 7.5-15 mg/kg intramuscularly used in 4 studies
Netilmicin/kanamycin used in other studies
Given the age of the studies included, no plazomicin was used
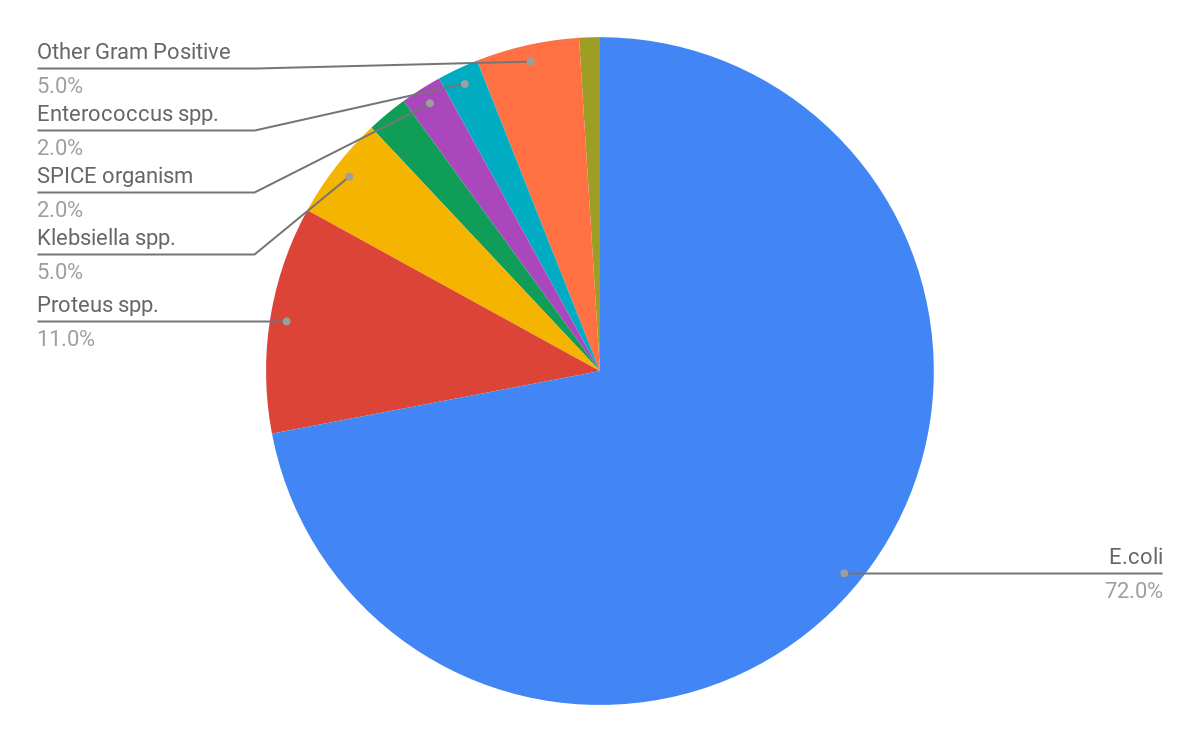
Pathogens Isolated
Efficacy
Outcome
Result
Microbiologic cure(11/13 studies)
94.5%
Clinical cure(2/13 studies)
82.8 – 94.7%
30 day recurrence rate
19% (equal number reinfection vs relapse)
Initial microbiologic cure rate- Anatomic abnormality vs no abnormality
86.3% vs 96.9% (p<0.01)
Sustained microbiologic cure at 30 days- Anatomic abnormality vs no abnormality
57.3% vs 87.5% (p<0.001)
Microbiologic cure- pediatric vs adult studies
95% vs 94% (p>0.05)
Initial microbiologic cure rate- AG vs Comparator
95.4% vs 95.6% (p=0.71)
Sustained microbiologic cure at 30 days- AG vs Comparator
71.0% vs 72.8% (p=0.76)
Safety
64 of 13,804 patients experienced adverse effects (0.5%) in the single dose AG group
7 nephrotoxicity
53 vestibular toxicity
3 patients with injection site discomfort
1 transient paresthesia around the mouth
The comparator groups experienced an adverse event rate of 3.5
Limitations
13,258 of the 13,804 came from a single study
Old studies
Clinical cure infrequently evaluated due to limited symptom data
Comparator group did not include nitrofurantoin, a drug of choice for lower cystitis today
Dosing of comparator antibiotics not readily available
Author’s Conclusion
Existing evidence provides support for single-dose aminoglycoside therapy as a plausible treatment for cystitis in adults and children.
Some Thoughts
Excited about further incorporating this into practice as an option for patients with lower UTI and compliance issues, multidrug resistant pathogens, or multiple allergies precluding the use of other agents. I’ll also be utilizing it for people who simply are willing to receive injection(s) right here in the ED to complete therapy. (similar to those wanting Penicillin G for Group A Strep pharyngitis).
Gentamicin will be the primary AG to reach for given many of the studies utilized it, it is less costly then amikacin, and our local susceptibilities show excellent gram-negative susceptibilities. Tobramycin may be an option if your local susceptibilities support this as superior to gentamicin given similar pharmacokinetics and pharmacodynamics.
I’ll be giving preference to 5 mg/kg of gentamicin/tobramycin or 15mg/kg of amikacin to ensure adequate exposure until more studies are conducted on lower doses.
The 2 studies that used single dose AG for pyelonephritis showed promising initial cure rates, however were small. It’s reasonable to use caution and mostly avoid this indication until more data is available.
Use caution when considering this approach in patients with anatomical abnormalities. While these patients inherently have lower cure rates and higher relapse rates, comparative data from this systematic review show significantly lower initial and sustained microbiologic cure.2
Utilize adjusted body weight in those >120% of their ideal body weight, and prepare them for multiple injections as the dose likely needs to be split into multiple syringes.
If You Read Nothing Else
Gentamicin 5mg/kg IM x1 dose appears to be a safe and effective option to treat lower urinary tract infections among pediatric and adult patients.
Avoid use in patients with sepsis, bacteremia, and significant renal insufficiency.
Pyelonephritis and patients with anatomical abnormalities are a grey area, use caution and ensure close follow up if utilizing single dose AG for this.
Goodlet KJ, Benhalima FZ, Nailor MD. A Systematic Review of Single-Dose Aminoglycoside Therapy for Urinary Tract Infection: Is It Time To Resurrect an Old Strategy? Antimicrob Agents Chemother. 2018 Dec 21;63(1)
Minardi D, d’Anzeo G, Cantoro D. Urinary tract infections in women: etiology and treatment options. Int J Gen Med. 2011;4:333-43.



You must be logged in to post a comment.