
BCEMP content coming soon
More to come.
More to come.
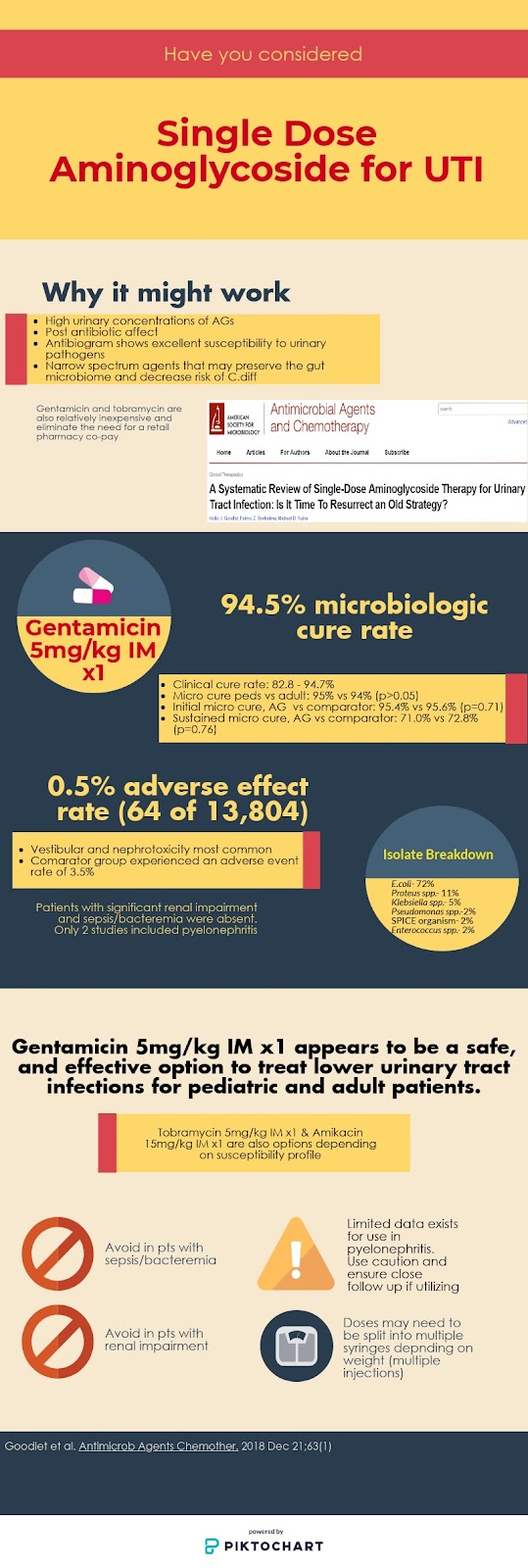

Looking for a single dose, no compliance issues, inexpensive, safe, and effective option to treat urinary tract infections? An older therapeutic option might be the answer. A recent systematic review by Goodlet et al. looks into the utility of single dose aminoglycosides (AGs) to treat cysitis.1
Article
Design
Results
Population
Intervention
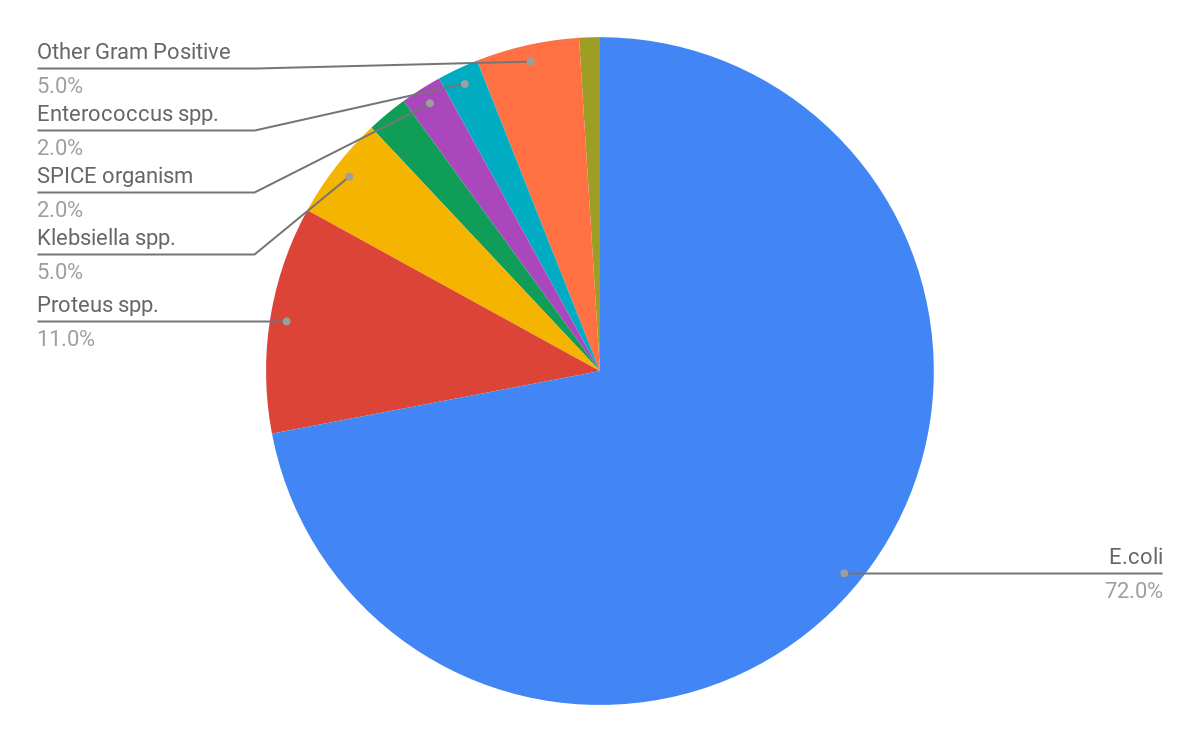
Pathogens Isolated
Efficacy
| Outcome | Result |
| Microbiologic cure(11/13 studies) | 94.5% |
| Clinical cure(2/13 studies) | 82.8 – 94.7% |
| 30 day recurrence rate | 19% (equal number reinfection vs relapse) |
| Initial microbiologic cure rate- Anatomic abnormality vs no abnormality | 86.3% vs 96.9% (p<0.01) |
| Sustained microbiologic cure at 30 days- Anatomic abnormality vs no abnormality | 57.3% vs 87.5% (p<0.001) |
| Microbiologic cure- pediatric vs adult studies | 95% vs 94% (p>0.05) |
| Initial microbiologic cure rate- AG vs Comparator | 95.4% vs 95.6% (p=0.71) |
| Sustained microbiologic cure at 30 days- AG vs Comparator | 71.0% vs 72.8% (p=0.76) |
Safety
Limitations
Author’s Conclusion
Some Thoughts
If You Read Nothing Else
Tony Mixon, PharmD, BCPS, BCIDP
References
Zahra Nasrazadani, PharmD, BCPS
Emergency Medicine Clinical Pharmacist
Salina Regional Health Center
A few months ago, Kristina Kipp wrote her inaugural EMCrit article enumerating her (extremely justified) concerns with the data we had available at the time regarding andexanet alfa…or should I say “coagulation factor Xa (recombinant), inactivated-zhzo”(1)? Since then—and in a somewhat perverse order of operations—the drug has been rolled out in a second-generation release and later, the New England Journal of Medicine published the final results from Portola’s ANNEXA-4 trial (2). Essentially, the results revealed what most of us expected to see. There is no need to re-adjudicate the conclusions Dr. Kipp reached in her manifesto to righteous cynicism. Now, the question becomes— what do we do with this information? My recommendation is the same that I brought to our Pharmacy and Therapeutics Committee: keep the drug off of formulary, at least for now. What follows is a compendium of the strategies I found useful at our institution, compiled in one convenient article for your viewing pleasure.
A Review
First, I’d strongly encourage you to read Dr. Kipp’s original post on the subject of andexanet last June (3). It covers a lot of the bedrock clinical concerns that we should be keeping at the forefront of our opposition.
Andexanet’s primary mechanism of action is via binding and sequestration of Factor Xa inhibitors—specifically apixaban and rivaroxaban—to reverse their anticoagulant effects. The sequestered anticoagulants are unable to perform their Xa-inhibitory functions and anti-Xa levels decline quickly; they then recover and possibly rebound around an hour after the drug’s two-hour infusion is completed (4,5). What does that mean? Well, we still don’t know. Measuring anti-Xa levels is a fairly common surrogate endpoint for determining hemostasis, yet our ANNEXA-4 authors conclude that “there is no significant relationship between hemostatic efficacy and reduction in anti-factor Xa activity during andexanet treatment,” based on the analyzed data. Therefore, all hemostatic efficacy endpoints were determined clinically by an adjudication committee whose “members were blinded to the extent possible in a single arm cohort study.” And although that tricky little detail has been widely pulled into the light of day for scrutiny, it really cannot be over-emphasized: ANNEXA-4 had no comparator group. More to come on that point in a bit. Let’s dig into the persuasive bits.
Clinical Evidence
So what do we use instead of andexanet? This isn’t a problem to be solved—our normal standard of care is already firmly in place and quite effective. Although off-label, prothrombin complex concentrate (in the US, usually of the 4-factor variety, 4F-PCC) has been a handy little workhorse for this purpose.
If you’re crafting your formulary, start with an evaluation of the way your institution utilizes 4F-PCC. How many patients do you reverse annually overall? How about specific to the direct oral anticoagulants (DOACs) in question, apixaban and rivaroxaban? You’ll need this data to assign hard numbers to pharmacoeconomic analysis, but you also can’t establish a starting point for this conversation without knowing your current state of affairs. Look at the pertinent metrics: hemostasis, dose, subsequent thrombotic events, etc. Is your institution using the the drug-reference-recommended 50 units/kg dose? Ours implemented a lower dose regimen at 25 units/kg a couple of years ago and we’ve found our in-house results to be consistent with the published literature on the matter, which is to say: it works. Because dose-finding studies weren’t performed to bring this drug to market, many studies have attempted to do some post-market analysis with promising results at much lower doses.
A 2016 executive summary of antithrombotic reversal recommendations from the Neurocritical Care Society and the Society of Critical Care Medicine recommends 50 units/kg for DOAC reversal (6). The following year, the UPRATE trial found that a 25 unit/kg dose was sufficient to achieve 69% anticoagulant reversal with a low rate of embolic events at 2.4% (7). When evaluating intracranial hemorrhage in 2018, Schulman et al found similar efficacy and safety with this low dose (8). Whichever dosing strategy your institution chooses, you have clinical support for doing so. The 2016 reversal guideline above, paired with the American College of Cardiology expert consensus in late 2017 both provide formal support for utilization of 4F-PCC in DOAC reversal (9). If you worry that these guidelines don’t include andexanet references because it came to the market after their publication, the American Heart Association has you covered. In early 2019, their journal, Stroke, published a summary of current approaches and included both andexanet and 4F-PCC as treatment choices for DOAC reversal (10).
As pharmacists, we’re often not thinking about the risk of litigation, and certainly it’s not looming over us the way it is for physicians. They need to know that your formulary recommendations aren’t putting them at increased risk just as much as they need to know about clinical risk to your mutual patients. By providing guideline-level evidence to support your formulary choice, you’ll be able to assuage some of this concern. Use the evidence cited above to show them that they will not be failing to meet the standard of care by choosing to make andexanet unavailable, and that’s an important fact as well as key phrasing and framing for your argument.
So far, what we’ve done is assess our status quo and build evidentiary support for 4F-PCC in DOAC reversal. If you’re sports-minded, this is called defense and it’s not enough to win an argument. You also need to develop some offense. It’s the difference between “what we’re doing is good” and “the alternative is demonstrably bad.” Andexanet was approved and delivered to market via the FDA’s Accelerated Approval Program. As such, Portola is not required to assess meaningful, patient-centered outcomes. They need only “fill an unmet medical need on whether the drug has an effect on a surrogate or an intermediate clinical endpoint” (1). Ostensibly, this explains away the lack of a comparator group. Although much has been said about ANNEXA-4’s significant limitations, it bears repeating that this study also utilized exclusion criteria such that they limited the study only to the healthiest patients. They chose subjects that could feasibly be managed without reversal of their anticoagulants. Although I believe andexanet should be kept off of your formulary, you may be faced with a physician or physician group that insists on the drug’s availability. If you simply can’t avoid purchasing this drug, it is in our patients’ best interest to insist that the same exclusion criteria be implemented as restrictions on andexanet’s use. It has not been studied in the sickest bleeding patients and still experienced a surprisingly high all-cause mortality rate at 30 days. As Dr. Justin Morgenstern notes, “if [andexanet] is given in a population of patients you don’t expect to die, 14% will die” (11).
As a reminder, exclusion criteria include: patients needing surgery within 12 hours, intracranial hemorrhage with a Glasgow Coma Score of less than 7, hematoma volume greater than 60 mL, expected survival less than one month, thrombotic event in the two weeks prior to enrollment, or receipt of warfarin, dabigatran, or various blood products (PCC, recombinant factor VIIa, whole blood, plasma) within the prior 7 days. Doesn’t that list sound very much like the patients for whom you’d most want and need a reversal agent? The surgeons at your institution think so, too. And although those exclusion criteria are extensive, ANNEXA-4 also didn’t enroll patients with “visible, musculoskeletal, or intra-articular bleeding.” They also didn’t permit discretionary doses of andexanet beyond the approved bolus and two-hour infusion. To enforce all of these parameters at your institution, you’ll need to frame utilization of andexanet as analogous to alteplase in ischemic stroke. Work through the checklist, determine your patient’s eligibility, and try to make your electronic health record pull its weight. It quickly becomes cumbersome and unrealistic but we have no idea what andexanet would do to those excluded patient populations so it is essential to protect them.
Although we’ve talked quite a bit about clinical considerations already, we haven’t even tackled hemostatic efficacy yet. So, does andexanet alfa work? The answer is that we actually still don’t know. Patient’s in the ANNEXA-4 trial were assessed for hemostasis at 12 hours after the end of their andexanet infusion. To be included, their last DOAC dose had to have been no more than 18 hours prior to treatment. So, let’s say a patient took their DOAC precisely 18 hours ago, then received a 15-30 minute bolus of andexanet, and then a 2 hour infusion. Study subjects could be as much as 20.5 hours out from their last DOAC dose when the 12-hour clock starts ticking, which means they are 32.5 hours out at the first analyzed assessment of hemostasis. With half-lives of 12 hours and 5-9 hours for apixaban and rivaroxaban, respectively, there is no appreciable drug still on board when this assessment was performed for at least some percentage of patients. By choosing a chronologically distant endpoint, the authors of ANNEXA-4 aren’t asking a meaningful question in the first place.
So, we have an off-label agent that works well and has lots of available evidence, plus the backing of expert guidelines to support its use. And we have another agent with one poorly-designed study and no useful outcome measures. So we’ve established some solid defense and a key piece of offense: our cherry-picked patient population—that explicitly was only included when expected survival was greater than one month—actually generated a number needed to harm of approximately 7. On to the next.
Pharmacoenonomic considerations
When andexanet alfa was initially released to selected sites, before we even knew much about its efficacy, everyone seemed to know that this drug was expensive. In healthcare, much of the cost of our interventions is woefully lacking transparency. Drug pricing charts circulated rampantly in the FOAMed Twittersphere painted an impossible picture in the order of tens of thousands of dollars. Now that any institution can order andexanet, we can confirm the rumors by querying our wholesaler. At the time of writing, andexanet is $22,000 per package of four 200mg vials. Any hospital wishing to keep andexanet in stock should keep three flats on hand at all times in order to be adequately stocked to administer the high-dose regimen, which is an 800mg bolus plus a 8 mg/min infusion for 2 hours, which totals 960mg. At a cumulative dose of 1760mg, that is a $66,000 out-of-pocket expense; accountant friends might chime in with something about cash flow. And depending on how often you are reversing DOAC bleeds, it’s possible you’ll be throwing nearly $70K in the garbage when it outdates. Remember the good old days when we thought 4F-PCC was costly?
The pharmacoeconomic angle is perhaps the easiest piece of this discussion to make compelling. For my institution, our annual cumulative 4F-PCC expenditure was less than the cost of treating just two high-dose andexanet patients. If you take this information to your P&T Committee, know that you won’t just be speaking to physicians. In general, these decision-making bodies also include administrators and various C-suite types. They speak the language of dollars, whereas we tend to speak the language of pharmacokinetics and chemistry. Know your audience and tailor a piece of your presentation to the more financially-minded individuals in the room. Consider also the payment structure for the vast majority of anti-coagulated patients—that is, predominantly Medicare recipients. Patient stays are reimbursed based on their assignment into a diagnosis-related group (DRG). In 2016, the average covered charge for an intracranial hemorrhage ranged from $26,728 to $53,754. GI bleeds were covered from $20,910 to $50,999, with the actual dollar amount depending on the ICD-10 code that is applied to each patient. And although these are the “covered charges,” the actual Medicare payouts range from $4,485 to $13,097, again depending on the diagnosis (12). Now, I’m no accountant, but the very fact that this is not the language I normally speak is what necessitates our involvement in the financials. We’re looking at massive sums that, when not fully covered, become the responsibility of the patient. The details are extremely complicated so these dollar signs don’t perfectly account for all of the moving parts, but the gap between what’s paid and what’s incurred is not one that can be spanned by minor adjustments. These numbers are simply staggering.
If you are making the case for keeping andexanet off of your formulary or applying rigorous restrictions, know that you aren’t alone. Get in communication with your group purchasing organization and find out how other institutions are handling this formulary decision. At the point where other massive and famous health systems are keeping andexanet off of their formularies (and they are), your hospital’s leaders are going to be reassured that they are making a decision somewhat multilaterally. Your purchasing organization is a wealth of information and is a valuable tool when making formulary decisions overall. For example, our institution’s purchasing group is conducting a survey of all participating hospitals regarding andexanet formulary decisions and will disseminate this information to members to bolster the conversations they know we’ll need to be having. Plus, your C-suite types are generally very compelled by this kind of information because they know other suits have thoroughly vetted their decision as well.
Scientific integrity
ANNEXA-4 sets a dangerous precedent if we allow it to do so. However, I don’t believe the study is wholly without merit. For one thing, it provides evidence for something many of us suspected all along: anti-Xa levels might not really mean much. For another thing, it is an excellent educational tool for learners of all varieties. This would be a great journal club article because it allows a student or resident to learn how to truly lay bare the “limitations” section of their presentation.
If you’ve been dying for the perfect illustration of the pitfalls of surrogate endpoints, now is your moment. Conversations about the importance of appropriate blinding are also warranted. The ANNEXA-4 authors offer a single line dedicated to justifying the total lack of comparator group: “At the time of study initiation, it was determined that a randomized, controlled trial would have logistic and ethical challenges, given the perceived risks of placebo assignment in this highly vulnerable population.” Even assuming we allow this assertion (but please don’t), they offer no explanation whatsoever as to why the comparator couldn’t have been the usual standard of care. Lacking this control group, the study is unable to reach conclusions about one of the most fundamental evidentiary concepts: statistical significance. Was the hemostasis achieved by andexanet significant? We can’t know. And that’s not just because of the lack of a comparator, but because they study also didn’t meet power. Importantly, the sample size of 350 patients required to meet power was determined, in part, by regulatory requirements that necessitated more patients in each DOAC group, beyond the initially planned 250 patients. Although the authors state that 250 patients would have been enough to meet power, the increased sample size suggests that the FDA disagreed. Ultimately, however, only 254 patients made it into the efficacy population and only 249 were included in analysis. So, by neither the first power calculation nor by the amended requirement was power met.
The line following the smoke and mirrors about unethical placebo groups is even more telling: “However, continued use of unapproved agents, despite a lack of rigorous clinical data, has changed the equipoise for a trial.” Again, the authors are setting up some fallacious arguments but also showing their hand. Use of 4F-PCC does have reasonably strong clinical data behind it (several examples of which they cite in their own references) but more importantly, no “rigorous clinical data” was collected by this trial. Additionally, this statement, when translated to plainer English, says, “off-label use of 4F-PCC showed us a money-maker niche so the balance of forces or interests has shifted.”
This is also a good moment to demonstrate the importance of reading the supplementary materials. There are all sorts of hidden gems lurking, and if your learners don’t already make a habit of deep-diving into the background and supporting literature when they present journal clubs, now is the time to enforce that practice. From the supplement, we learn that our hand-picked healthy patients were supposed to have been a very different group, but the exclusion criteria were extensively modified as the study progressed. Another noteworthy change includes adjusting the hemostatic efficacy assessment time from 24 hours to the 12 hours used in the study. The originally-planned 24-hour timeline would put the first assessment of hemostasis as far out as 44 hours from the last DOAC dose; this amendment was made “based on regulatory feedback.” The supplement also discloses the difference in hemostatic effect when comparing patients who received low versus high dose andexanet regimens. Although the statistical significance is unclear, high-dose patients numerically had poorer (or no) hemostasis than those who received low doses; we might interpret this to mean that patients who still had drug in circulation at the initiation of treatment were more poorly reversed than those patients in whom the DOAC dose was smaller and more chronologically distant. So, it seems we still have not answered the efficacy question.
TL;DR
Overall, this conversation covers a lot of ground. It’s intended to be a good spread of the variety of folks that are represented at your institution’s P&T. These are just some of the strategies that were useful at my specific institution. You may find yourself presenting the same information to more focused physician groups, like trauma or surgery sub-committees. Do some politicking in advance and assess who is already on your side or at least receptive to the conversation. Treat curbside questions about that new bleeding reversal drug as a golden opportunity to spread the good word of 4F-PCC and plant the seeds of well-placed skepticism at the ANNEXA-4 methods. Develop an elevator speech that hits the high points:
Folks who insist on andexanet availability will make assertions based on what they hope the drug will accomplish. As you’ve seen, these are not founded in the data, so push back with confidence and diplomacy.

You must be logged in to post a comment.